Savinib+Oshitinib seven -line therapy MET patients with advanced pulmonary adenocarcinoma, PFS over 9 months
Author:Cancer Channel of the Medical Time:2022.08.16
*For medical professionals for reading reference

Wonderful cases of lung cancer sharing, one -click check!
This case is a 53 -year -old female patient with advanced right lung adenocarcinoma, accompanied by right pulmonary, septum, dual -collarbone region lymph nodes metastasis, bone, liver, and brain mostly metastasis, and right lung obstructive pneumonia and right thoracic effusion. The first diagnosis was the EGFR 19DEL mutation. After the first line was treated with Ekitinib, it was resistant to medicine. There was no progressive survival (PFS) for 11 months. The second -tier treatment was changed to Osteini targeting therapy, and disease progress (PD) occurred 11 months later. From November 2020 to September 2021, patients with three to six lines received treatment schemes such as standard chemotherapy and antiovascular generic drugs. Essence
In October 2021, the patient performed a liquid droplet digital PCR (DDPCR) gene test. The results were displayed as MET amplification. In 9 months, it is still under treatment and actively follow -up. The case was provided by Professor Huang Zhangzhou, Fujian Cancer Hospital, and invited Professor Zhuang Wu, a Fujian Cancer Hospital for review.
Profile
Basic situation: Patient women, 53 years old, were first admitted to the hospital for the first time on November 2, 2018 because of "repeated cough and chest tightness for more than 20 days".
Past history: hepatitis B surface antigen carrier.
History of medical: There is no obvious history of smoking and no obvious smoke. The causes of paroxysmal cough and a small amount of white phlegm, clinic at Sanming Second Hospital.
Chest+sinus CT: The right frontal lobe occupies, it is recommended that MRI, the right horny position may be, the longitudinal lymph nodes, the right pneumonia, the right thoracic effusion, and the multiple occupy in the liver.
Chest+abdominal CT: right lung central lung cancer, two -collarbone region, right pulse lymph nodes metastasis and right lung obstructive pneumonia and right thoracic effusion; multiple metastases in the liver.
Skull MRI: Multiple transfers of the skull.
The whole body bone ECT: The radioactive distribution of the sternum handle and the fourth rib on the right, and the bone metastasis is considered.
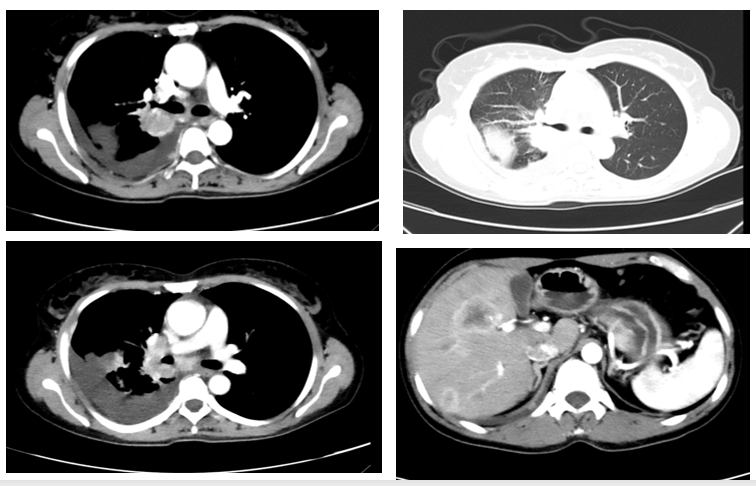
Patient baseline chest+abdomen CT
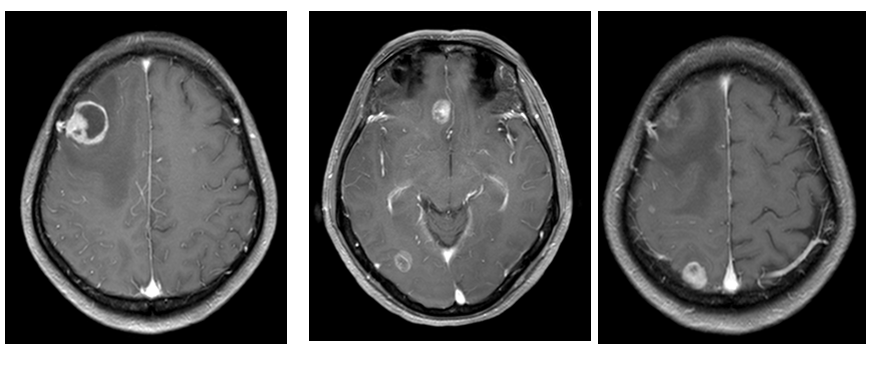
Patient baseline head mRI
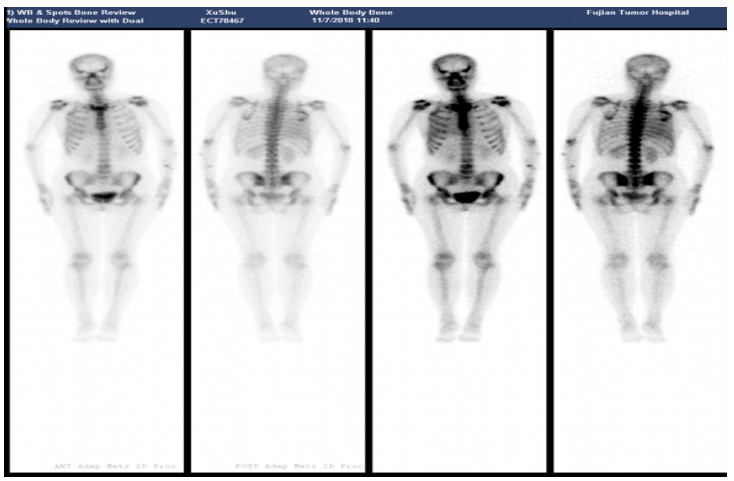
Patient baseline system bone ECT
Pathological: (bronchial biopsy) adenocarcinoma. IHC: K7+, Napsina+, TTF-1+, P40-, P63, KI67 about 60%+.
Pulmonary tissue second -generation sequencing (NGS): EGFR 19DEL (50.5%).
Diagnosis: Right lung adenocarcinoma with right hindow, mediastinal, dual -collarbone region lymph nodes metastatic bone, liver, brain migration and right lung obstruction pneumonia and right thoracic effusion CT2N3M1C IVB stage (EGFR19DEL, ALK, ROS1 wild type).

The patient was diagnosed with lung adenocarcinoma with right honeycomb, hypertrophy, dual -collarbone region lymph nodes metastatic bone, liver, brain migration and right lung obstructive pneumonia and right thoracic effusion (CT2N3M1C IVB stage), EGFR 19DEL mutation. Therefore, the first-line therapy selects a generation of EGFR-TKI EGFR-TKI Egenni-targeted therapy and cooperates with the whole brain's palliative radiotherapy. The efficacy assessment is PR, and the PFS is 11 months. In November 2019, the primary stove of the patient's lungs made a slight progress, and the second -tier was treated with Osteini targeting, and the target was not detected by the blood gene test.
In August 2020, the primary and liver metastases of the patient's lungs made a slight progress, and Oshitininib combined with Bervarzumab was treated until October 23, 2020. In November 2020, the patient reviewed CT to show the progress of the tumor, and the patient began to receive Peime Quzer+Card Platinum+Bevarzab three -line treatment. Three -line treatment is not effective, and rapid progress after 1 cycle. On December 18, 2020, patients received the four -line treatment of Dorcio. The best effect was SD and PFS was 3 months. In March 2021, the patient reviewed MRI, and the divestitudes of the brain increased more than before. From March 30, 2021 to August 4, 2021, the patient received 4 cycles for the treatment of Arotinib in combined with the five -line treatment of Niogo.
In September 2021, patients with primary stoves, liver metastases, and adrenal metastases were progressing. Therefore, they accepted the 1 cycle of Ameitinib and Arotinib six -line targeted therapy. Due to the significant increase in creatine kinase, Aceitinib was stopped. Essence In October 2021, the patient received the MET amplification gene detection and used DDPCR to detect the blood of the patient. The results showed that the patient's MET amplification (copy number 2.6), seven -line therapy has received the treatment The efficacy assessment is SD.
Provide experts
Professor Huang Zhangzhou: In the era of precision treatment, dynamic gene test helps patients with advanced lung cancer patients throughout the process
With the rapid development of genetic testing technology, the diagnosis and treatment of non-small cell lung cancer (NSCLC) has undergone tremendous changes. For patients with EGFR mutations, EGFR-TKI is a standard first-line treatment method. In this case, the EGFR 19DEL mutation was first diagnosed. The first-line therapy adopted an EGFR-TKI drug Egfr-TKI drug Ekitinib therapy to reach PR, and the PFS was 11 months. However, in the treatment process, such patients will inevitably occur. Studies have shown that one of the drug-resistant mechanisms after EGFR-TKI treatment during MET is expanded. %-21%[1-2], the incidence rate after three generations of EGFR-TKI is 15%-30%[3-4]. At the same time, inhibiting MET and EGFR may be a treatment strategy for MET amplification after EGFR-TKI resistance. After multi -line treatment, the patients in these cases have progressing rapidly since the second -line treatment, and the efficacy is not good. After that, the patient performed the blood DDPCR gene test, and the results were displayed as MET amplification. The patient's seven -line receiving MET inhibitor Savinib+Oshitinib has been treated with good control. The tumor SD has been in good control. The PFS has reached 9 months. It is still under treatment and active follow -up. It can be seen that the treatment plan for Savininib+Oshitinib has brought good treatment benefits to patients with advanced lung cancer treated with this type of ultra -back line.
The treatment of this patient has shown that the treatment process of NSCLC patients who drive gene positive NSCLC should be dynamically detected for multiple times to better choose targeted treatment plans for patients, achieve the purpose of precise treatment and full management, extend the survival of patients to survive time.
Expert Reviews
Professor Zhuangwu: EGFR-TKI drug-resistant patients with metamorphosis with MET amplification in the ultra-rear line, Saverninib+Oshitinib effectively controls the condition and helps patients to extend their survival
Reported in the past shows that for the EGFR-TKI-resistant crowd caused by MET amplification, MET-TKI combined with EGFR-TKI is an effective treatment strategy. High -selective MET inhibitors Savigini's approval has broken the "no medicine available" therapeutic dilemma of MET amplification, bringing new treatment options for such patients. TATTON Research [5] explored the efficacy and safety of MET enlarged patients after the treatment of EGFR-TKI for the treatment of EGFR-TKI for the treatment of EGFR-TKI. In the MET amplification crowd, the treatment of Savinib+Oshitinib can still bring 33%of the objective relief rate (ORR) and 5.5 months of PFS, in addition to good tolerance. This reminder, even for patients with multi -line therapy, Savacinib and Oshitinib can still bring curative effects and safety benefits.
In this case, the EGFR 19DEL mutation was first diagnosed. After the first-line and second-line EGFR-TKI targeted therapy, the patient inevitably faced the dilemma of EGFR-TKI. It can adopt schemes such as standard chemotherapy, antiovascular generation drugs or radiotherapy, and the effect is not satisfactory, and the multi -line solution fails.
After multi -line treatment, the patient detected MET amplification through the DDPCR detection method, and then received Savidininib combined with Oshitinib for treatment. The condition was well controlled, and there was no obvious side effects and good tolerance. Patients are still being treated and actively follow -up. This once again verifies the efficacy and safety of the treatment and safety of Savidinib combined with Oshitinib.
At the same time, clinicians are also reminded that MET amplification is a common drug resistance mechanism for EGFR-TKI targeted therapy. Clinically, it needs to pay attention to MET amplification testing. Although the MET amplification detection is currently preferred by the FISH detection, the blood NGS, DDPCR and other detection methods can be considered due to the failure of the tissue specimen.
It is expected that in the future, high-efficiency and low-toxic drugs such as Savininib can continue to conduct clinical research and bring greater benefits to EGFR-TKI patients with drug resistance.
Comment expert introduction
Professor Zhuangwu

Administrative Director and Chief Physician of the Internal Medicine of the Cancer Hospital of Fujian Province
Deputy Chairman of the Precision Medical Branch of Chinese Elderly and Elderly Medical Society
Standing Committee Member of the Chinese Physician Society of Cancer Multi -disciplinary Diagnosis and Treatment Committee
Academic Member of the Chinese Academy of Lung Cancer
Member of the TLCR Oncology Consultant Committee
Standing Committee Member of the Professional Committee of the Pulmonary Cancer of the Fujian Provincial Anti -Cancer Association
Member of the China Medical Care International Exchange Promotion Association of Lung Cancer Prevention and Control Branch
CSCO esophageal cancer professional committee member
Deputy Chairman of the Fujian Maritime Association of Tumor Clinical Diagnosis and Treatment Branch
Executive Member of the Beijing Cancer Prevention Research Association
Standing Committee of the China Precision Medical Professional Committee
Executive Member of the Rehabilitation Branch of the Chinese Medical Association for Elderly Medical Association
Executive Member of the Fujian Maritime Association Tumor Prevention and Control Association
Standing member of the Fujian Provincial Taihai Medical Association
Executive Member of the Chinese Medicine Association Cancer Drug Research Committee
Member of the International Cancer Research Association (IASLC)
"Oncology Magazine" executive editorial board
Introduction to experts
Professor Huang Zhangzhou

Deputy Chief Physician of the Department of chest oncology of Fujian Cancer Hospital
Member of the 2nd Cancer Internal Medicine Committee of the Fujian Anti -Cancer Association
The second and third youth committee members of the Professional Committee of the Fujian Anti -Cancer Association
Councilor of the Chinese Medicine Association Cancer Drug Research Committee of China Chinese Medicine Association of Chinese Medicine Association
Member of the Professional Committee of Pan -Delta chest tumor alliance
Pan -long triangular chest tumor alliance professional committee non -small cell lung cancer rare target target group member
Member of the first small cell lung cancer in Fujian Province
Member of the precision medical professional committee of the Fujian Strait Tumor Prevention and Control Science and Technology Exchange Association
Member of the First Rehabilitation Committee of the Fujian Anti -Cancer Association
Director of the Clinical Oncology Diagnosis and Treatment Branch of the Fujian Straits Medical and Health Exchange Association
references:
[1]. Pasquini G, GiaccoNe G. C-MET Inhibitors for Advanced Non-Small Cell LUNG CANCER [J]. Expert Opin Investig Drugs. 2018; 27 (4): 363-375.
[2].Bean J, Brennan C, Shih JY, et al. MET amplification occurs with or without T790M mutations in EGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib[J]. Proc Natl Acad Sci U S A. 2007;104 (52): 20932-7.
[3].Ramalingam SS, Cheng Y, Zhou C, et al. Mechanisms of acquired resistance to first-line osimertinib: preliminary data from the phase III FLAURA study. 2018 ESMO Congress. Abstract LBA50.
[4] .wang y, li l, han r, et al. Clinical Analysis by Next-Generation Sequencing for NSCLC PATIENTS with MET AMPLICICIONT to Osimertinib [j]. LUNG CANCER.
[5].Lecia V Sequist, Ji-Youn Han, et al. Osimertinib plus savolitinib in patients with EGFR mutation-positive, MET-amplified, non-small-cell lung cancer after progression on EGFR tyrosine kinase inhibitors: interim results from a Multicentre, Open-Label, Phase 1B Study [J]. Lancet Oncol. 2020; 21 (3): 373-386.
*This article is only used to provide scientific information to medical people, and does not represent the viewpoint of this platform


- END -
Heilongjiang's latest epidemic notice
At 0-24:00 on June 17, 2022, there were no new local new crown pneumonia epidemic ...
Xinle City Dis -determined that a community is a mid -risk zone

Notice on delineation of new crown pneumonia risk areasXinle Changshou Street Xinx...