What do you think of this uterine endometrial cancer?Come and learn!
Author:Cancer Channel of the Medical Time:2022.08.16
*For medical professionals for reading reference

Unlifted/de -divorced endometrial cancer pathological characteristics and differentiation diagnosis
I. Overview
Undealized uterine endometrial cancer is an invasive pathological subtype of endometrial cancer, accounting for about 2%-9%of endometrial cancer. The incidence is higher than transparent cell carcinoma. In 2006, Silva was first named. Malignant epithelial tumors lacking gland sample differentiation and non -fixed -type growth, lack of or rare neuro endocrine differentiation.
Unlimized cancer can be associated with low -grade endometrial cancer, and the term "de -differentiated cancer" is applied. Before the female genital tract tumor 2020 WHO, de -differentiated cancer is strictly defined as an unlimized cancer and low -level endometrial cancer (FIGO1 and level 2). At present, high -level endometrial cancer can also occur in de -differentiated cancer. Aggressive biological behavior.
2. Clinical characteristics
The average age is 50-55 years old, mainly showing postmenopausal bleeding. Most of them are progressing during diagnosis. A few patients have a history of rectal cancer. Some cases have family history related to Lynch syndrome.
Third, general features
Typical manifestations are large polypic lumps (2-15cm) in the uterine cavity. They are usually filled with the entire uterine cavity. Most tumors are located in the uterine body. Individuals are located in the lower section of the uterine.
Fourth, mirror characteristics
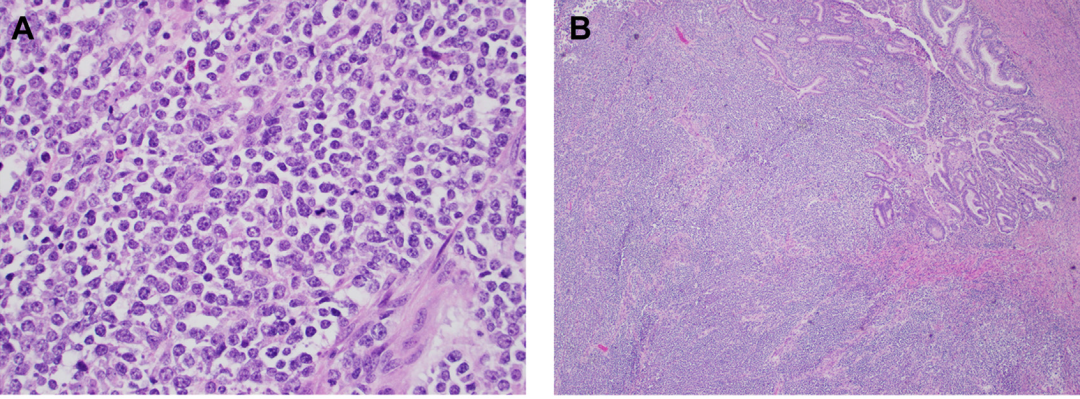
Unlimized endometrium cancer, whether simply or as an ingredient of dehuminating cancer, is characterized by the pervasive distribution of non -adhesive epithelial cells (Figure 1A), which is mostly medium -sized and distributed. It is round or polygonal, an empty nucleus, and occasionally obvious nuclear kernels. The multi -shape is not obvious or only small stoves appear. The cytoplasm is small and occasionally enrich the cytoplasm. It often shows a wide range of map -like necrosis, lymph blood vessel invasion and significant tumor infiltration lymphocytes (40 per 10hpfs & 40, averaged 95).
It can also be seen that horizontal muscle -like cells or pulp cell -like cells can be seen. It can be seen that there will be sudden keratinization of mucus samples. Typical de -differentiated cancer is characterized by sudden transformation of undifferential cancer and low -level uterine endometrium (Figure 1B).
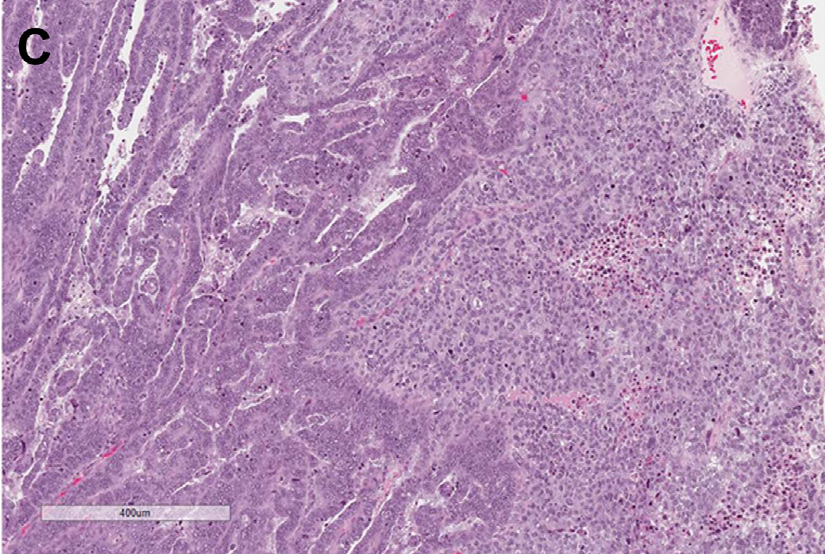
High -level endometrial cancer components (Figure C) can also appear in the background of undifferentiated cancer, including endometrial samples, transparent cells, and slurry, and high -grade tumor morphology may also be a different type of hybrid cancer.
5. Immunization
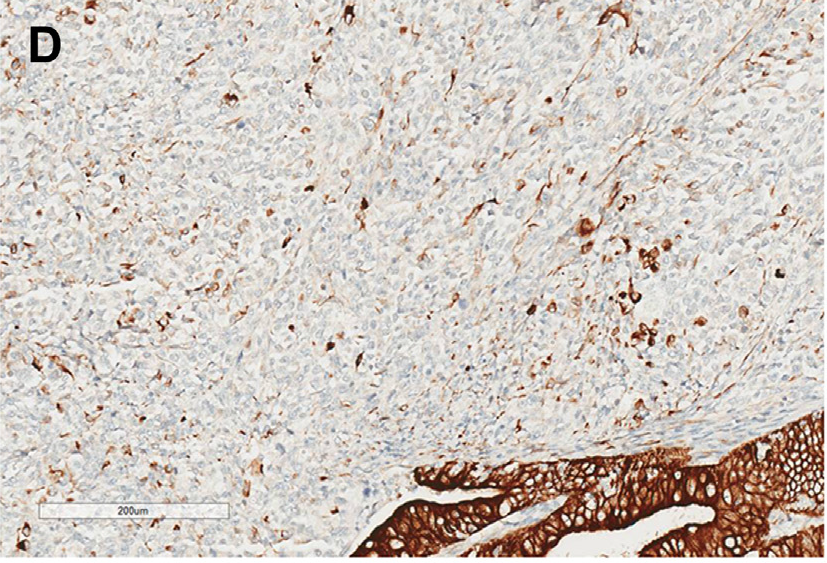
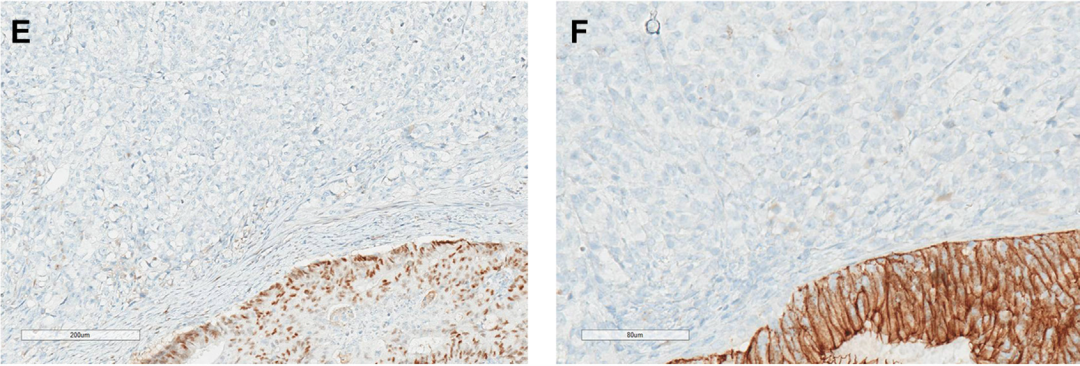
Broadcasting CK (Figure 1D), CK8/18 and EMA often manifested as negative, nuclear or bureau stove but strong positive (<10%). ER and PR are generally negative (Figure 1E), Vimentin and ZEB1 are always positive, E-Cadherin is usually negative (Figure 1F) or inning the stove yang. PAX8 is usually negative (80-90%case). Claudin4 is usually negative.
About 30%of SMARCA4 lost expression, while INI1 was expressed in 5-10%cases. In de -differentiated endometrial cancer, SMARCA4's loss of expression is mainly limited to undifferential cancer components. The horizontal muscle -like shape is not expressed without SMARCA4/INI1. Claudin-4, PAX8, ER and PR negatives in SMARCA4/INI1 missing expressions are more common.
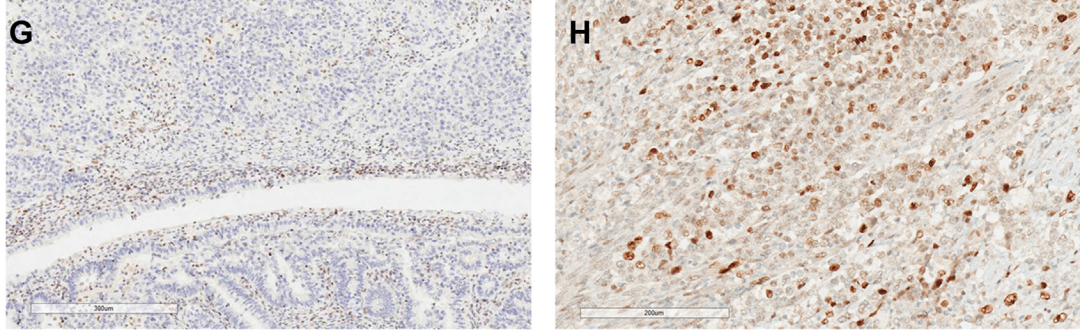
MMR protein deficiency expression is usually lack of MLH1 and PMS2 (45-70%cases), and most of them are caused by MLH1 methylation. Defamation of cancer is often deficient in tumor components (Figure G).
Unlifted or de-divorced endometrial cancer may occur in P53 abnormal expression (15-30%cases). However, most of them are P53 wild-type expression (Figure H). Some studies believe that P53 abnormal expression is related to SMARCA4/INI1 mutation.
Studies have found that 50%of the case CyClind1 is permeated with strong positive, and 30%of the cases express CD34, 34%of cases are filled with P16. SYN and CGA are usually negative or positive. According to the International Association of Obstetrics and Gynecology, in non -differentiated cancer, the nerve endocrine marker should be <10%tumor cell positive.
Six, molecular features
There are differences in de-differentiated cancer and undifferentiated cancer TCGA endometrial cancer molecular types. MSI type/high mutation subtype is more common in dehuminating/undifferentiated cancer (40%-60%). MLH1 launching MLH1 and PMS2 lack of MLH1 and PMS2 is the most common, and Pole/ultra-mutating subtypes are also relatively high (11.0%-15.9%).
A considerable part of the mutant genes of endometrium -like cancer are usually also occurred, such as PTEN, PIK3CA, CTNNB1, TP53, and POLE nucleic acid slicing enzymes. In addition, SWI/SNF complex protein often occurs. Usually SMARCA4 (35%) loss or SMARCB1 (10%) mutations excludes each other, and some mutations include Arin1A/Arid1b (25%).
7. Differential diagnosis
The most important identification diagnosis of de -differentiated cancer is endometrial adenocarcinoma and cancer sarcoma. Unlimized cancer needs to be identified with the following diseases, including: high -level endometrial cancer, Smarca4 lack of uterine sarcoma, high -level endometrial tartar, malignant melanin, malignant melanin Tumor, lymphoma, high -level nerve endocrine cancer.
Identification 1: Uterine endometrial -like cancer
Definitive/undifferentiated endometrial cancer ratio ratio 3 endometrial -like cancer survival rate (25%VS60%). If the latter grows and/or tissue fixation, the adhesiveness can be similar to undifferentiated cancer, but it has it. The gonad -like structure, the cells of the solid region are similar to the composition of the gland, and most of them form a clear cable, small beam -shaped or group distribution. The lack of cell adhesion and glandular formation of non -differentiated cancer ingredients, and horizontal muscle -like structures can be seen. Immunization: Normally CK/EMA is usually lacking or the expression of the stove, PAX8/ER/PR/E-Cadherin is negative, INI1 or SMARCA4 is missing, and endometrium-like cancer usually expresses the above indicators. However, in special circumstances, a small number of unlimized cancer PAX8 and ER can be expressed, while advanced endometrial cancer can be missing.
Identification 2: SMARCA4 lack of uterine sarcoma
SMARCA4 is missing the morphology of uterine sarcoma and undifferentiated cancer, including epithelial cells, horizontal muscle -like shapes, non -adhesive cell growth, necrosis, significant lymph vascular violations and Smarca4 lack. The former mainly occurs in young women and can appear leaf -like structure similar to glandular sarcoma, while the latter mainly occurs in women who are scaled or after menopause. If there is obvious nuclear nuclearity, it indicates that the endometrium cancer is not differentiated.
Sabialarous sarcoma is usually P53 wild type, MMR is normal, CK, EMA, Claudin-4 is usually negative, molecular detection can help identify diagnosis.
Identification 3: High -level endometrial interstitial sarcoma
Among the high-level endometrium intravascular sarcoma, it is accompanied by YWhae-Nutm2 fusion with uniminatiated cancer. They all have the characteristics of nuclear split and active epithelial-like cell morphology. PR is usually negative, and Cyclind1 can also be expressed in 50%of uniminaged cancer cases, and molecular detection can help identify diagnosis.
Identification 4: Cancer Harm
Differentiated cancer and cancer sarcoma are displayed under low -power mirrors, showing the characteristics of mucus -like inter -type. It can also be seen that heterosexual differentiation.
Aptiflasm cells can be seen, but it should be a stove. Cancer sarcoma is usually abnormal in P53 mutation or immunohistochemistry, normal expression of MMR protein, and stable microbesin.
references:
Liu Yan, Zhang Kun, Liu Yingrong. Go/Divide the Progress of Clinical Pathology of endometrial cancer [J]. Chinese Pathological Magazine, 2022, 51 (7): 682-686
Mirkovic J. Uncommon and Difficult High-Grade EndometRial Carcinomas. Surg Pathol Clin. 2022 Jun; 15 (2): 301-314.
Obstetrics and gynecology pathology: upper, lower volumes/Zheng Wenxin and other editors.-2 version .- Beijing: Science Press, 2021.10
First of this article: The pathological channel of the medical community
Author of this article: Tian Liang
Audit expert: Professor Dong Lin, Cancer Hospital of the Chinese Academy of Medical Sciences
Editor in charge: Sweet
- END -
For three consecutive days, Chengdu Zero Zero Zero

Local epidemic special reportAt 0-24 o'clock on August 9th, there were no new loca...
Is it painful?Experts teach you the secret to deal with headaches

In order to further popularize the culture of traditional Chinese medicine health,...