In the era of precision treatment, how to do colorectal cancer diagnosis?
Author:Cancer Channel of the Medical Time:2022.08.29
*For medical professionals for reading reference

This article focuses on the pathological diagnosis part of the latest 2022 version of colorectal cancer, and compares it with the NCCN guide and ESMO guide.
This article focuses on the pathological diagnosis part of the latest 2022 version of colorectal cancer, and compares it with the NCCN guide and ESMO guide, including morphological examination, immunohistochemical dyeing and molecular pathological testing.

Scan the two -dimensional code above and get more tumor guidelines information
1. Biopsy specimen
The biopsy specimen contains endoscopic biopsy and puppet puncture biopsy. All specimens should be fixed in time (fixed in 30 minutes). Use a fresh 3.7%neutral buffer formaldehyde fixed solution. 8 ~ 48 hours.
1
General inspection
Grade I recommendation: Organizational size and number.
2
Mirror inspection
Grade Ⅰ recommendation: Clarify the lesions and types, tumors/non -tumors, benign/malignant, organizational types (refer to the WHO digestive system tumor classification 2019 version), and tissue grading.
3
Immunohistochemistry
Grade Ⅰ Recommendation: Mismatch Repair (MMR) protein expression.
Grade II recommendation: The detection of immunohistochemical markers used to identify diagnosis. According to the purpose of identification, the typical immune phenotype of colorectal gland cancer is CK7-/CK20+/CDX2+.
4
Molecular pathological test
Class I recommendation: Microsatellite Instability (MSI). Judgment standard is level 3:
MSS (Microfex stable)
All 5 digits are stable
PMMR
MSI-L (low-degree unstable of microfinee)
1 bit of unstable
PMMR
MSI-H (Microcarmatic height is unstable)
Two or more sites are unstable
DMMR
5
Compared with NCCN and ESMO guide
This part of the three version of the guidelines is consistent.
Second, adenoma local resection specimen
Local resection specimen of adenoma contains circles, endoscopic mucosal resection, and endoscopic mucosal dissection, all specimens should be fixed in time. In addition, the specimen should be fully expanded by the endoscopic or surgeon, and the mucosa surface should be fixed on the cork or foam plate on the edge of the specimen on the edge of the specimen. The whole material should be cut vertically every 2 to 3mm on the mucous membrane surface.
1
General inspection
Grade Ⅰ recommendation: tumor size, there is pirate/non -si.
2
Mirror inspection
Grade Ⅰ recommendation:
Clarify the type of adenoma; when the alien hyperplasia/epithelial tumor variable level (high level/low level) is accompanied by infiltrated cancer, it is necessary to clarify the histological type, organizational grading, infiltration depth, side cutting edge and base cutting edge, vascular violations , Tumor buds. The related concepts are as follows:
Adinet with infiltration cancer
Aginoma contains adenocarcinoma (PT1) that penetrates the mucous membrane muscle layer infiltrated to the lower layer of the mucosa (PT1)
Adenoma with high -level epidermal internal tumor changes
Adventory with severe hyperplasia, in situ cancer and intramuscular cancer
Tumor germination
Infiltrate the front edge of the infiltration of the side, a single tumor cell scattered in the interstitial or the cell cluster of the cells of ≤4 tumor cells
A 20-fold eye mirror (0.785mm) is selected under a hot spot for tumor buds for tumor buds, 0-4 is level I (low level), 5-9 levels 2 (medium-level), ≥10 are level 3 (high height (height (high level)
3
Immunohistochemistry
Grade Ⅰ Recommendation: MMR.
Grade II recommendation: The detection of immunohistochemical markers used to identify diagnosis.
4
Molecular pathological test
Grade Ⅰ Recommendation: MSI.
5
Compared with NCCN and ESMO guide
(1) Definition of positive cutting fate:
NCCN guide
1) Tumor distance <1 mm; 2) Tumor distance <2 mm; 3) Tumor cells are within the heat therapy range of cutting edge.
CSCO guide
The tumor distance is <1 mm.
(2) Hall characteristics related to bad prognosis:
ESMO guide
1) lymphatic or intravenous violations; 2) level 3 divide; 3) obvious tumor buds (& level 1).
CSCO guide
1) Vercular violations; 2) High -level adenocarcinoma; 3) 3) 3) tumors buds; 4) Tumor distance is less than 1mm.
Third, cure specimen
The cure specimen is usually fixed after cutting the intestinal tube along the tumor side. It is recommended to fix the nail plate, and the fixed steps are the same as above.
1
General inspection
Grade Ⅰ recommendation: specimen type, tumor site, intestinal length, general type of tumor, tumor size, tumor distance on both sides, no perforation, all rectal membrane division (TME) system The number, size, and grouping of lymph nodes.
(1) TME specimen system membrane integrity evaluation standard:

(2) Lymph nodes are taken in the direction of lymphatic flow (beside the intestine, middle, and central). The cure specimens that are not treated with neo -assisted treatment are not less than 12 in principle. If 12 lymph nodes are not found for the first time, re -examination is recommended.
2
Mirror inspection
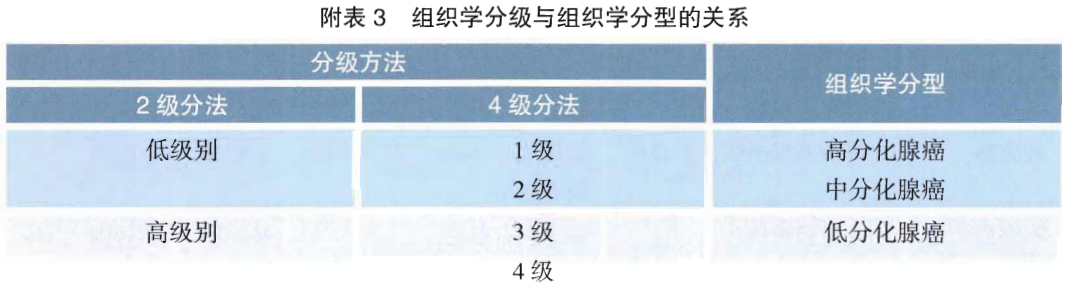
Grade I recommendation: organizational type, organizational grading, infiltration depth, vascular violation, neurological violations, two sides of cutting edge, circular cutting edge, total number and total number of lymph nodes, number of cancer nodules, tumor germination, TNM staging, tumor retreat Grade (TRG). (1) The tissue classification includes the traditional 4 -level method and the 2nd grade method of the class classification, which is based on the degree of glandular formation.
(2) "Conditioning edge" refers to the "base" cutting edge without the intestinal wall covered with peritoneum. It is recommended that the surgical physician paint or identifies at the circular edge of the ring. "Conditional edge positive" refers to the ≤1mm of the tumor distance from the edge of the tumor.
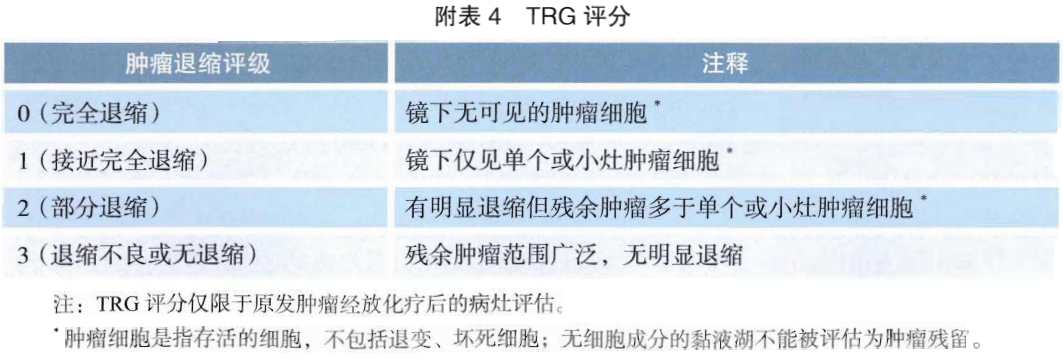
(3) The pathological assessment of tumor retreat grading (TRG) is analyzed based on residual tumor composition and fibrosis. It is recommended to use AJCC's 8th edition TRG scoring system.
3
Immunohistochemistry
Grade Ⅰ Recommendation: MMR.
Grade II recommendation: The detection of immunohistochemical markers used to identify diagnosis.
4
Molecular pathological test
Grade Ⅰ Recommendation: MSI.
Class II recommendation: RAS and Braf gene mutations detection, detection sites include V600E of KRAS and NRAS genes No. 2, 3, 4, and V600E of BRAF genes.
5
Compared with NCCN and ESMO guide
(1) The NCCN guide focuses on the concept of isolation tumor cells and micro -transfer in this part:
Isolated tumor cells
IHC or single tumor cells detected by multiple HE levels and/or <0.2 mm tumor cell clusters.
Micro
Tumor cell blocks with diameter ≥0.2 mm and ≤2 mm or cell clusters of 10-20 tumor cells are deemed to be standard positive lymph nodes (PN+).
(2) The ESMO guide lists the main and secondary prognostic parameters of Phase II risk assessment in this section. Main prognostic parameters: resection lymph nodes <12; PT4 installment includes perforation. Smaller parameters: high -level tumors; blood vessel infiltration; lymphatic pipe infiltration; peripheral nerve infringement; obstruction; high level CEA level before surgery.
Fourth, metastatic colon cancer surgery/biopsy specimen
1
General inspection
Grade Ⅰ Recommendation: Specifications for the same root.
2
Mirror inspection
Grade Ⅰ Recommendation: Specifications for the same root.
3
Immunohistochemistry
Grade Ⅰ Recommendation: MMR.
Grade III recommendation: HER-2.
4
Molecular pathological test
Class I recommendation: MSI; RAS and BRAF gene mutations detection.
Grade III recommendation: NTRK fusion detection.
5
Compared with NCCN and ESMO guide
The ESMO guide also refers to chemotherapy sensitivity/toxic prediction logo.
Patients who are used to be used in patients with a dysherazine dehydrogenase (DPD) before the use of 5-尿 fluoropicidine.
UDP glucosaminylase altering enzyme 1 family polypeptide A1 (UGT1A1) phenotype detection is recommended for patients (low bilirubin) for UGT1A1 missing, and the dose of Ilonaron is more than 180 mg/square Patients of rice.
The above is a general point of pathological diagnosis in the CSCO guide of the latest 2022 colorectal cancer.
First of this article: The pathological channel of the medical community
Author of this article: Xu Jianhao
Audit expert: Professor Dong Lin, Cancer Hospital of the Chinese Academy of Medical Sciences
Editor in charge: Sweet
- END -
Latest release!Announcement on the trajectory of 2 positive infected people outside the province in the province in Taiyuan City
Notice of the Office of the Leading Group for the Prevention and Control Work of the New Coronatte Pneumonic Pneumonia Epidemic Extraction of Taiyuan City(No. 74, 2022)Notice on the trajectory of 2 po
Crossing 1,000 kilometers of heart protection journey!22 -year -old college student "changed his heart" to be reborn

Wuhan Evening News June 22 (Correspondent Ning Yafei reporter Li Qing) The 22 -yea...