How does MET abnormal NSCLC diagnose and treat?The latest Atorg expert consensus point is here
Author:Cancer Channel of the Medical Time:2022.09.06
*For medical professionals for reading reference

Sworing one by one and understanding MET abnormal NSCLC diagnosis and treatment points!
Non -small cell lung carcinoma (NSCLC) is a very heterogeneous disease with a lot of driving gene mutations, including MET abnormalities. Recently, the Asian chest tumor research group (ATORG) has formulated an expert consensus on MET abnormal diagnosis and treatment, let us see it!
1. The best meta mutation detection method
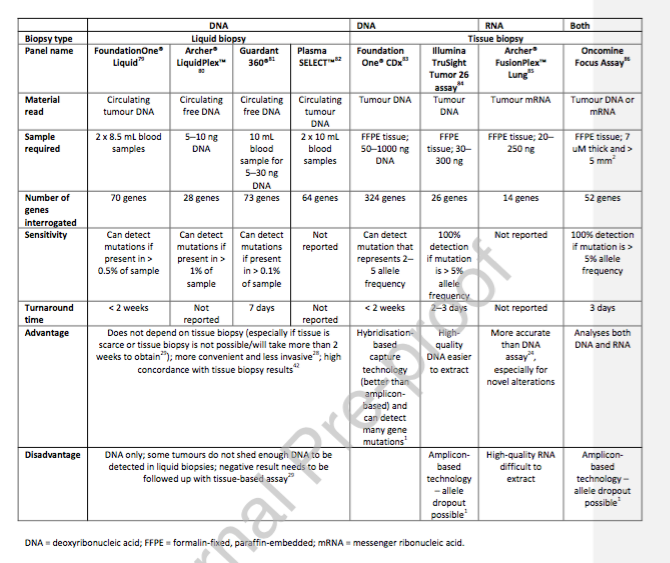
Question 1: What is the best detection method for the best detection method of MET14 outer Xianzi jumping mutation?
ATORG Consensus: It is recommended to test the detection of met14 outer sub -jump mutations in patients with late NSCLC. Because each platform and technology are constantly developing, and in different clinical environments, the availability and detection methods are different in different clinical environments, so Atorg does not specify the best detection method, but it is clearly stated that the out -of -MET14 out -of -MET14 out -of -the -art sub -appendage The detection of jump mutations should be arranged based on the detection of the availability, the characteristics of the detection, the possibility of positive, the condition of the patient's disease, and the optional treatment method. In the NSCLC multi -genomic detection, the detection of exposure and jump mutation of MET14 should be preferred. Of course, arranging orthogonal tests according to the patient's situation may be useful.
Table 1: A list
Question 2: What are the best means for MET amplification detection?
ATORG Consensus: The gold standard of MET amplification detection is fluorescent in situ hybridization (FISH). Of course, new technical means are also constantly emerging and gradually become available. For example, using tissue biopsy or circulatory tumor DNA (CTDNA, liquid biopsy) in the plasma sample to monitor the MET gene copy (GCN).
2. The current status of the treatment of jumping mutations and guidance suggestions of Met14
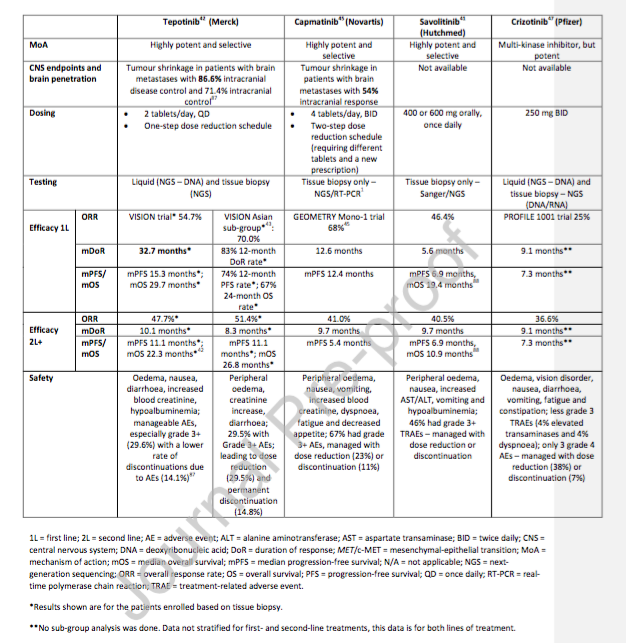
Question 3: What are the currently available MET inhibitors and what factors affect the formulation of treatment decisions?
Atorg consensus: China Savacinib (the only approved at present in China) and TEPOTINIB, Capmatinib (not approved in China) can be used as first, second, or back -line treatment of patients with migrants in MET14. When waiting for gene test results, patients can still use standard (SOC) chemotherapy. If high -selective MET inhibitors are not available, Kazidinib can consider choice as a second -line or back line.
Table 2: Drugs available for jumping mutations in MET14
Question 4: For patients with high expression of PD-L1 high expression and MET14 out-of-appearance jump mutation, how many MET inhibitors are considering using MET inhibitors during the treatment?
ATORG Consensus: There are already random control studies, and the comparison of MET inhibitors and SOC (chemotherapy and/or immunotherapy) with two advanced NSCLC patients with two hybrid phenotypes or hybrid physics characteristics. The treatment of combined chemotherapy is still the standard treatment of such patients, especially during first -line treatment. Although retrospective studies have shown that the PD-L1 expression of patients with jumping mutations in MET14 will increase, the treatment response seems to have nothing to do with the expression of PD-L1, and it is related to the lower medium tumor mutation load (TMB). However, more clinical research data still needs to give any clear suggestions. During the second -line treatment, if the drug is available, the MET inhibitors should be targeted. After the progress of the disease, biopsy and genetic testing should be carried out repeatedly to clarify the latest genetic mutations and then guide the treatment.
3. MET amplification in EGFR-TKI drug resistance
Question 5: What role does the MET amplification in EGFR-TKI resistance played?
ATORG Consensus: EGFR-TKI is the standard therapy for EGFR mutations late NSCLC. The previous research results indicate that after the EGFR-TKI first-line treatment, patients with the progress of drug resistance due to MET amplification have a good treatment effect using EGFR-TKI combined with MET inhibitors. However, before more data appear and the drug can be further improved, patients who have obtained EGFR-TKI obtaining drug resistance due to MET amplification are treated with chemotherapy as a standard treatment. Of course, doctors need to adjust the treatment plan according to the patient's situation and the treatment of toxicity. In addition, ATORG recommends that patients with EGFR-TKI obtained drug resistance will be included in the clinical study of the combined treatment of EGFR-TKI obtaining drug resistance.
Question 6: How should I choose the right biomarker in clinical research?
ATORG Consensus: Most clinical studies of the combined treatment of hyper-selected MET inhibitors and EGFR-TKI are phase I/II clinical studies. It should be considered that FISH testing is mainly included in clinical research. FISH can perform MET amplification detection, and NGS covers a wider detection range. It can accurately infer the MET GCN and can be used to detect a variety of drug -resistant mechanisms, and then play more role in MET detection. For patients with EGFR-positive NSCLC who have progressed after EGFR-TKI's first-line treatment, it is not recommended to test MET amplification. However, for patients with EGFR positive NSCLC who use Oshitinini as a second -line therapy for the choice of T790M mutations, they may progress due to secondary meta amplification. Therefore, the sub -group of the patient should conduct MET amplification testing. Fourth, MET detection and metability of MET inhibitors
Question 7: What is the availability of daily MET detection?
Atorg consensus: At present, the challenges of MET detection mainly include plans that lack standardization and non -state funding. The test selection is mainly based on the availability of local MET testing and whether there is a clinical trial. ATORG suggested that Met14 outer exposure -jump mutation should be a key choice for multi -gene detection.
references:
[1]Myung-Ju Ahn, Marvin Jonne L. Mendoza, Nick Pavlakis, et al. Asian Thoracic Oncology Research Group(ATORG)Expert Consensus Statement on MET alterations in NSCLC: Diagnostic and Therapeutic Considerations.
First of this article: Rare target ecosystem in the medical community
Organize this article: Tumor Baby
Editor in charge: Sweet
- END -
Sale and recall nationwide!20 batches of medicines do not meet the requirements
According to the State Drug AdministrationThe Institute6 pharmaceutical inspection institutions testMark as Zhengzhou Ruilong Pharmaceutical Co., Ltd., etc.9 companies produced by companies, etc.20 ba
The market supervision bureau of Jinchuan County, Sichuan Province continues to carry out the prevention and control of epidemic conditions in the market supervision field

On August 31, the Jinchuan County Market Supervision and Administration Bureau con...