Good medicine first, drug-resistant worry-free 丨 Osicinib first-line drug resistance-Her2 amplification/mutation response strategy
Author:Cancer Channel of the Medical Time:2022.09.19
*For medical professionals for reading reference

Osicinib is a weapon for lung cancer treatment. The corresponding drug -resistant treatment scheme can be adopted for different drug resistance mechanisms.
As the third generation of EGFR-TKI, the emergence of Oshitinib solved the problem of drug resistance of the first-generation/second-generation EGFR-TKI and became the "life-saving straw" of countless EGFR mutations positive non-small cell lung cancer (NSCLC) patients. At the same time, with the announcement of Flaura's research results, the first -line treatment of Oshitinib broke the historical records of the non -progressive survival period (PFS) and the overall survival (OS), which significantly extended the patient's survival time. However, Oshitinib treatment will inevitably appear to resist.
Previously, we have shared with you the main drug resistance mechanism of Osicinib, C797S and MET amplification strategies. This article will continue to introduce the occurrence and solution of HER2 amplification/mutation after the first line of Oshitinib for treatment. Let the clinicians "worry -free", rest assured that "good medicine first", and eventually better benefit the majority of patients with lung cancer.
Osicinib first -line treatment, refresh PFS and OS historical records
Flaura Study is a phase III clinical trial of random, control, multi-center, and double-blindness, aiming to explore patients with Oshitinib to compare the first-line EGFR-TKI first-line treatment of EGFR mutations positive or metastatic NSCLC patients. The main endpoint is PFS evaluated by researchers, and OS is the key second point.
From Flaura's research data, it can be seen that compared with a generation of EGFR-TKI, the first-line treatment of EGFR mutations in the treatment of EGFR mutations is significantly extended to PFS to 18.9 months, and the risk of disease progress or death by 54%(HR = 0.46, 95%CI: 0.37-0.57), and each Asian group has benefited [1]. In addition, the median OS of Oshitinib for 38.6 months has broken through the longest OS record of EGFR-TKI single drug treatment [2].
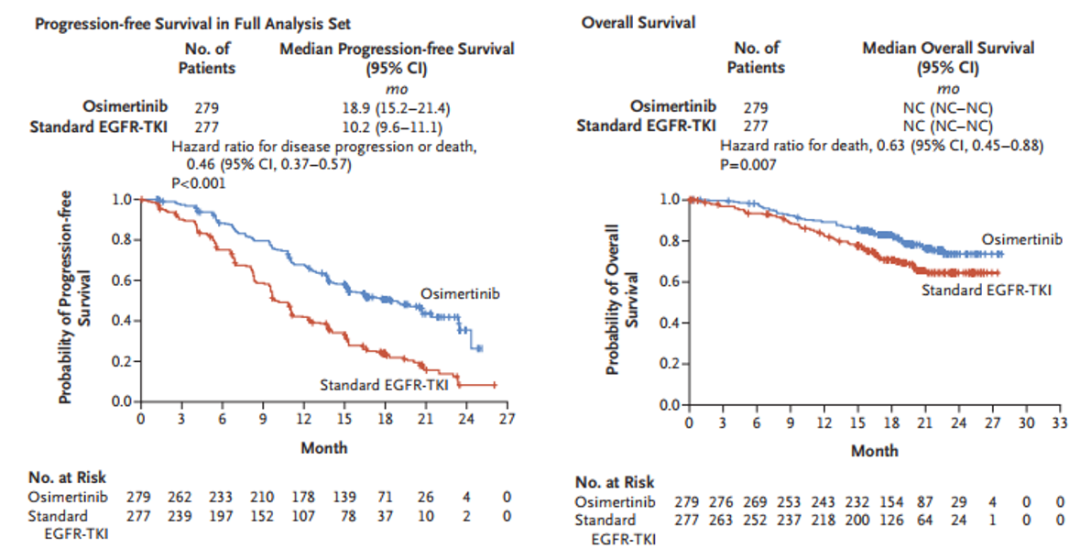
Figure 1. PFS and OS results for the first -line treatment of Osicinib in Flaura Research
Oshitinib also has an advantage in preventing the transfers of the central nervous system (CNS). For patients with CNS metastasis, compared with the generation of EGFR-TKI, Oshitinib significantly extended the median PFS to February, and reduced the risk of disease progress by 53%(P <0.001) [1].
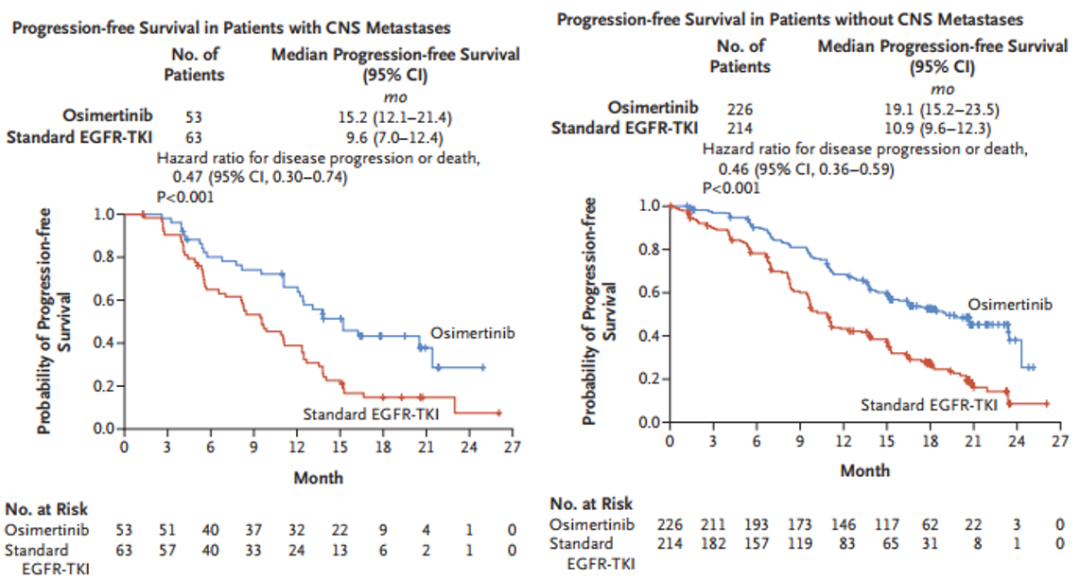
Figure 2. PFS and OS results of the first -line treatment of Oshitinib in Flaura studies in Flaura studies
At present, many domestic and foreign authoritative guidelines recommend Oshitinib as a standard first -line treatment plan for EGFR mutations positive patients. Among them, the National Comprehensive Cancer Network (NCCN) Guide is preferred. The highest score is recommended, the China Clinical Oncology Society (CSCO) guidelines are recommended by Class I.

Figure 3. Oshitinib first -line therapy is unanimously recommended at home and abroad guidelines
HER2 amplification/mutation and Oshitinib first -line treatment resistance
HER2 is a tyrosine kinase receptor and belongs to the EGFR family. Among different Her family proteins, Her2's catalytic kinase activity is the strongest [3,4]. Its phosphorylation can lead to downstream activation of PI3-AKT, Mapk and ERK MET/MAPK. [5-7]. HER2 mutations mainly include two forms of amplification and mutation in NSCLC, which will cause HER2 activation [8].
HER2 mutation is the carcinogenic drive gene of NSCLC, and it is also an important mechanism for EGFR-TKI to obtain sexual resistance. Clinical studies have shown that HER2 mutations are one of the Oxininib to obtain a drug tolerance mechanism. In the Flaura study, after the first -line treatment of Oshitinib, 2%of patients had HER2 amplification and 1%of patients with HER2 mutations [9]. In addition, AURA3 studies show that 5%of patients with Osicinib first -line treatment of HER2 amplification, and some patients have other target mutations [10]. However, in comparison, HER2 amplification is more common after the first-line treatment of EGFR-TKI (Eloatinib, Gefitinib), and the incidence rate is about 10%[11].
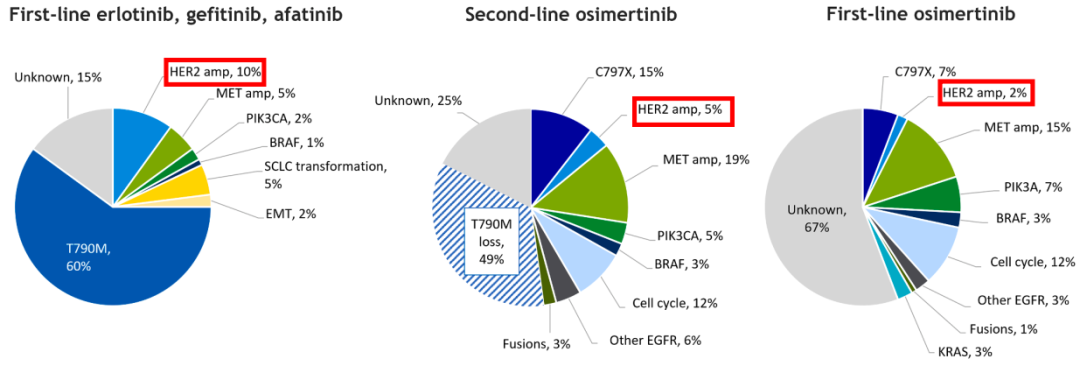
Figure 4. EGFR mutation NSCLC causes TKI drug resistance to mutations and amplification. [12]
See the trick, crack the Osicinib first -line treatment, HER2 amplification/mutation
So how to treat patients with advanced NSCLC patients with advanced NSCLC after the first -line treatment of Oshitinib for treatment? At present, many studies have been explored, and various treatments such as anti -HER2 monoclonal anti -resistance, TKI drugs and antibody coupling drugs (ADC) have shown better application prospects.
01
Anti -HER2 monoclonal resistance
A phase II and II phase study evaluated the efficacy and safety of Tushuzab combined with paclitaxel in the progress of EGFR-TKI for the progress of EGFR-TKI. And observed a 100%relief rate in patients with 4 cases of HER2 amplification (& 10 Copies/Nucleus) [13].
02
TKI drug
Pelotinib is an irreversible pan -Her tyrosine kinase inhibitor (TKI) with targets including EGFR/HER1, HER2 and HER4. A phase II study included 60 patients with Her2 20 exogenous appetizers and received at least one Phasein NSCLC patients who had a platinum -containing scheme chemotherapy. They were treated with 400 mg pyriginib daily. The results showed that piperinib single drugs have acceptable safety characteristics and promising anti -tumor activity, and ORR is 30%; the median PFS is 6.9 months, and the median OS is 14.4 months [14]. Phase II PATHER2 studies further explored the piperininib combined with anti -vascular production drugs Apetinib therapy HER2 amplification or late -mutation NSCLC. (DCR) 93.9%[15].
In addition, the stage II Zenith20-2 research shows that another Pan HER-TKI drug Poziotinib backline treatment HER2 No. 20 outer sub-expose NSCLC ORR is 28%, and the median PFS is 5.5 months [16].
03
ADC drug
Trastuzumab Emtansine (T-DM1) is an ADC drug composed of antibodies, non-cut connections, and effective loads. Dynasties of clinical studies show that T-DM1 may overcome Oshinininib tolerance [17]. A phase IIII study was included in patients who had been treated with EGFR-TKI in the past, giving T-DM1 treatment, and observed part of the alleviating (PR) of 4 patients with HER2 immunohistochemistry (IHC) 3+. The ORR was 20%. [18]. In addition, a phase II "Basket" study found that among 18 patients with HER2 mutant lung cancer who were treated with too many lines, the ORR treated with T-DM1 was 44%and the median PFS was 5 months [19].
Another ADC drug Trastuzumab Deruxtecan (T-DXD) also shows better anti-tumor activity in HER2 expression or HER2 mutant NSCLC patients. In a phase I study HER2 expression or HER2 mutant NSCLC patient queue, the ORR treated T-DXD was 55.6%and the mid-bit PFS was 11.3 months [20]. Studies on Phase II Destiny-Lung01 show that among the HER2 mutant NSCLC patients who have received the current standard treatment, T-DXD treatment is 55%of the ORR and the median PFS is 8.2 months [21].
In addition, the stage II Destiny-Lung02 Studies include non-scale NSCLC patients with non-regulatory or metastatic HER2 mutations that have previously treated diseases after general systemic treatment. T-DXD treatment is given. In the main efficacy analysis queue containing 52 patients, ORR was 58%and the mid -bit relief duration (DOR) was 8.7 months [22]. Based on the results of this research, T-DXD was approved by the US Food and Drug Administration in August 2022 to be used for HER2 mutations that have previously received systematic treatment. NSCLC's therapeutic drug.
04
other
In addition to anti -HER2 treatment, immunotherapy also shows a certain clinical activity in HER2 mutant NSCLC. A retrospective study found that the ORR of HER2 mutant NSCLC was 52%and the median PFS was 6 months [23].
HER2 No. 16 external jump jump is a new mechanism for Osteinini -resistant. In vitro studies have shown that Afutinib and Oshitinib can inhibit tumor cell growth and signal conduction [24,25].
Expert comment: A variety of new drugs and new plans have emerged, overcoming HER2 amplification/mutations Osicininibic tolerance prospects
HER2 amplification/mutation is an important mechanism for Oshitinini to resist. In the past, the treatment of such patients was mainly chemotherapy, but the effect was not ideal. At present, although the treatment of Obitinini -resistant HER2 amplification/mutations has not yet reached consensus, with the continuous research and development of various new drugs and new schemes, it has brought more choices to clinical treatment. For example, anti-HER2 monoclonal monopozab, TKI drugs pipinibicinibinib, Poziotinib, ADC drugs T-DM1 and T-DXD, immunotherapy, and Oshitinib combined schemes have already shown in clinical research. The prospect of anti-tumor activity, and T-DXD has been approved by the US FDA for HER2 mutant NSCLC treatment. In the future, we look forward to these new drugs and new schemes to carry out more research, and continue to accumulate evidence -based medical evidence of HER2 amplification/mutant NSCLC patients after Oshitininib to resist, providing guidance for clinical treatment.
Expert Introduction
Professor Cai Yong

Deputy director
Dr. Medical Doctor of Medical Master, Chief Physician
Executive Member of the China Pharmaceutical Education Association of the Lungs and Tumor Committee of the China Medical Education Association
Standing Member of the three -dimensional orientation committee of the China Lung Cancer Prevention and Control Alliance
Member of the Wu Jieping Medical Foundation Cancer Radiotherapy Committee
Song Qingling Foundation, Member of the World Chinese Cancer Association of the Chinese Cancer Association, Director Song Qingling Foundation of the Foundation of the Foundation of the Foundation
Member of the Precision Medical Branch of Chinese Elderly and Elderly Medical Society
Member of the Shanghai Anti -Cancer Association Radible and therapy Youth Committee
Member of Shanghai Medical and Health Youth Federation
references:
[1] .soria JC, OHE Y, VANSTEENKISTE J, et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell LUNG CANCER. N English. 2018 Jan 11; 378 (2). 113-125.
[2].S.S. Ramalingam, J.E. Gray, Y. Ohe, et al. Osimertinib vs comparator EGFR-TKI as first-line treatment for EGFRm advanced NSCLC (FLAURA): Final overall survival analysis. Annals of Oncology (2019) 30 (suppl_5 ): V851-V934.
[3] .hsu C-C, Et Al. Exon 16 – SKIPPING HEVEL MeChanism of Osimertinib Resistance in EGFR L858R/T790M – Positive Non – Small Cell LUNG CANCER. J. Thorac. Oncol.
[4] .Yan M, et al. R. Her2 Expression Status in DIVERSERSERS: Review of Results from 37, 992 Patients. Cancer Metastasis Rev. 2015, 34, 157–164.
[5] .planchard d, et al. Correction to: "Metastatic Non-Small Cell LUNG CANCER: ESMO Clinical Practice Guidnosis, Treatment and Follow-Up". Ann. ONCol. 0.07.
[6]. Laberti g, et al. Beyond egfr, alk and ros1: Current evidence and future perspectives on newly targetable onCogenic drivers in lung adenocarcinomo.
[7]. Paez J g, et al. Egfr Mutations in Lung Cancer: Correlation with Clinical Response to Gefitinib therapy. Science 2004, 304, 1497–1500.
[8] .midha a, et al. EGFR Mutation Incidence in Non-Small-Cell LUNG CANCER of Adenocarcinoma Histology: A Systematic Review and Global Map by Ethnicity. AM. J. CunCERII. 2911.
[9] .ramalingam s.s, et al. ET al. Mechaniss of acquired resision to first-line osimertinib: Preliminary data from the pHase III Flaura Study. Ann. Oncol. 2018, viii740.
[10].Papadimitrakopoulou V.A, et al. Analysis of resistance mechanisms to osimertinib in patients with EGFR T790M advanced NSCLC from the AURA3 study. Ann. Oncol. 2018, 29, viii741.[11].Wu SG, Shih JY. Management of Acquired Resistance to EGFR TKI-Thargeted Therapy in Advanced Non-Small Cell LUNG CANCER. Mol Cancer. 2018; 17 (1): 38.
[12].Johnson M, et al. Treatment strategies and outcomes for patients with EGFR-mutant non-small cell lung cancer resistant to EGFR tyrosine kinase inhibitors: Focus on novel therapies. Lung Cancer. 2022;170:41-51.
[13].de Langen AJ, Jebbink M, Hashemi SMS, et al. Trastuzumab and paclitaxel in patients with EGFR mutated NSCLC that express HER2 after progression on EGFR TKI treatment. Br J Cancer 2018; 119:558–564.
[14] .zhou c, li x, Wang Q, et al. Pyrotinib in her2-mutant advanced lung adenocarcinoma after platinum-back chemotherapy, open-label, single -RM. ; 38 (24): 2753-61.
[15].Yang G, Xu H, Yang L, et al. Efficacy and safety of pan-ErbB inhibitor pyrotinib combined with antiangiogenic agent apatinib for HER2-mutant or amplified metastatic NSCLC: a phase II clinical study. J Clin Oncol 2021; 39 (15 SUPPL): 9035.
[16]. Le X, Cornelissen R, Garassino M, et al. Poziotinib in Non-Small-Cell LUNG CARBORORINGHER2EXON 20 INSERTAON AFTER PRIRAPIES: Zenith20-2 TRIAL. -718.
[17].S. La Monica, D. Cretella, M. Bonelli, et al. Trastuzumab emtansine delays and overcomes resistance to the third-generation EGFR-TKI osimertinib in NSCLC EGFR mutated cell lines, J. Exp. Clin. Cancer Res . 36 (1) (2017) 174.
[18].S. Peters, R. Stahel, L. Bubendorf, et al. Trastuzumab Emtansine (TDM1) in Patients with Previously Treated HER2-Overexpressing Metastatic NonSmall Cell Lung Cancer: Efficacy, Safety, and Biomarkers, Clin Cancer Res 25 ( 1) (2019) 64–72. [19] .b.t. Li, R. Shenocore, et al. Ado-Trastuzumab Emtansine for Patients with Her2-Mutant LUNG CANGERS: Results from Aphase II Basket Trial, J. CLIN . Oncol. 36 (24) (2018) 2532–2537.
[20] .j. Tsurutani, H. IWata, I. Krop, et al. Targeting her2 with trastuzumab deruxtecan: a dose-expansion, Phase I Study in Multiple Advanced Solid Tumors, CANCER DISCOV, 2020.
[21] .b.t. Li, e.f. smit, et al. Trazumab deruxtecan in her2-mutant non-small-cell lung carncer, n engl j med. 386 (3) 241–251.
[22] .https: //////drugs/resourcess-Information-APPROGS/fda-Grants-accelerated-Approval-TRASTUZUMKAM-NXKIL2-Mutrant-Non-SMMANT-NON-NXKILERERAT lung
[23].Saalfeld FC, Wenzel C, Christopoulos P, et al. Efficacy of immune checkpoint inhibitors alone or in combination with chemotherapy in NSCLC harboring ERBB2 mutations. J Thorac Oncol 2021. S1556-0864(21)02292-9.
[24] .ofin M, SOMWAR R, Rekhtman n, et al. Acquired Alk and Ret Generations As Mechaanisms of Resistance to Osimrtinib in EGFR-Mutant Lung Cancers.
[25].Zeng L, Yang N, Zhang Y. GOPC-ROS1 rearrangement as an acquired resistance mechanism to osimertinib and responding to crizotinib combined treatments in lung adenocarcinoma. J Thorac Oncol 2018; 13:e114–e116.
*This article is only used to provide scientific information to medical people, and does not represent the viewpoint of this platform


- END -
Just released!Temporary static management in the two towns in Shilin County

On September 6th, the Epidemium Prevention and Control Command of Xilin County and...
1811 national high -risk zones!Heilongjiang Provincial Disease Control Release the latest epidemic prevention and control reminder

On September 1, the Heilongjiang Provincial Centers for Disease Control and Preven...