What are the updates of the European Lung Hypertension Guide in 2022?Professor Jing Zhicheng's interpretation | ESC2022
Author:Physician Daily Channel Time:2022.09.13
"Physician Daily Channel" follows us
Author: Jing Zhicheng, Department of Cardiology, Beijing Union Hospital
In 2022, the European Heart Society and the European Respiratory Society will jointly promulgate the new version of lung hypertension diagnosis and treatment guidelines after 7 years. The level of understanding and management of lung hypertension is important.
The Department of Cardiology, Beijing Union Hospital organized several clinical first -line doctors including Dr. Li Jingyi, Dr. Guo Fan, Associate Professor Jiang Xin, Associate Professor Xu Xichi, and other clinical first -line doctors. They summarized and shared with readers.

Professor Jing Zhicheng
01
Confirm the diagnosis of lung hypertension from the guide level
New standards for hemodynamics
1. The conference dynamic diagnostic standard for the first time of the conference dynamic diagnostic standard for the first time of the conference dynamic diagnostic standard for the first time of the conference dynamic diagnostic standard for the first time of the 6th World Symposium Hypension. Pulmonary Artely Pressure (MPAP) ≥25mmHg is reduced to> 20mmHg. The above standards have been proposed for more than 4 years, and have been widely recognized by the academic community.
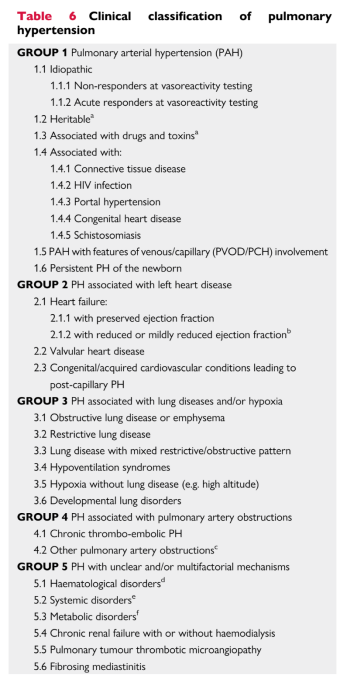
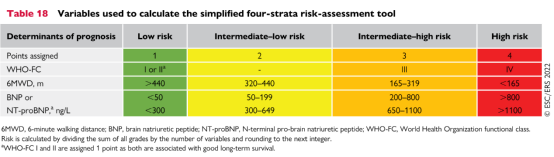
In 2022, the ESC/ERS Guide affirmed the new definition of lung hypertension and blood dynamics at the internationally widespread guide. The new blood dynamic diagnosis standards are closer to the pathophysiological characteristics of the lung circulation, which has an important role in promoting the early diagnosis of lung hypertension. Many patients with symptoms or asymptomatic critical lung hypertension (20mmHg However, the current lack of comprehensive evidence-based medical evidence of patient assessment, treatment and prognosis of patients with MPAP between 20-25mmHg requires a large-scale clinical study to further confirm whether early diagnosis and early treatment can improve the prognosis of these patients. 2. For capillary hypertension (mainly patients with 1, 3, and 4 patients with lung hypertension and part of the fifth largest category of lung hypertension), it is necessary to meet the following three blood dynamic standards to diagnose: MPAP> 20 mmHg, Pulmonary Arterial Wedge Pressure (PAWP) ≤15 mmHg and Pulmonary Vascular Resistance (PVR)> 2WU. In the past, the standard for rising pulmonary vascular resistance was 3 WOOD units, which have been reduced to 2 WUs, and the academic community requires that PVR elevation is the diagnosis of capillary anterior pulmonary hypertension. Pulmonary artery pressure caused by increased left heart disease, increased pulmonary blood flow, and increased thoracic pressure increase. The definition of hemodynamics further emphasizes the implementation of right cardiac duct examinations for patients with lung hypertension in clinical practice. It is necessary to determine the PAWP or left chamber diastolic pressure/left room pressure. It is believed that the concept of ultrasonic heart dynamics can be clearly diagnosed at least wrong. 3. There are also some patients with blood dynamic indicators in the clinic of MPAP> 20 mmHg, PAWP ≤ 15 mmHg, but PVR ≤ 2wu, although it meets the diagnostic standards of lung hypertension, does not meet the ahead of the capillaries or the pulmonary hypertension and blood pressure blood blood pressure blood blood pressure blood. Dynamic standards, which are called "unsugalted lung hypertension" in the 2022 ESC/ERS guide. The reason for the increase in MPAP in these patients is caused by the increase in pulmonary blood flow. It should actively screen whether there are relevant potential basic diseases in the clinic, such as congenital heart disease (especially room septal defects and pulmonary vein drainage) Conditional vein connection abnormalities, etc.), dynamic lapsea (liver, lung, brain and peripheral arteries), airway diseases, lung diseases and hyperthyroidism. 4. Exercise -related lung hypertension is also clearly defined as a blood dynamic state of lung hypertension in the 2022 version. It is defined as a cadiac output (CO) slope of MPAP/heart output after exercise. /L/min. It is clear that this definition is important for whether patients with short -term symptoms that are not explained after further use of invasive cardiopulmonary motion test assessment. 02 Supplement and adjustment of clinical classification 1. The 2022 ESC/ERS Lung Hypertension Guide follows the general framework of lung hypertension classification, and some sub -categories are supplemented and adjusted. 2. Divide special pulmonary hypertension (iPAH) according to the results of acute pulmonary vascular dilatation tests into two categories: the positive test of the acute pulmonary vascular dilatation test negative and acute pulmonary vascular dilatation test, but emphasized that individual genetic PAH and drugs or poison -related PAH are also emphasized. It may be positive as acute pulmonary vascular dilatation test. 3. Pulmonary occlusion (PVOD)/Pulmonic hemangioma -like hyperplasia (PCH) and neonatal persistent pulmonary hypertension (PPHN) are officially listed as 5 and 6 sub -sub -sub -categories of pulmonary hypertension. 4. Change the clinical category of the old version of the old version of the 2015 3 largest category of lung diseases/hypoxic dysfunction to a low ventilation syndrome, because simple hypoxic stalk resistance sleep disorders generally do not cause lung hypertension, and Patients with low ventilation syndrome often cause hypertonic hypertension during the day. 5. In particular, it is necessary to emphasize that: drugs recognized in the past that can be used for acute pulmonary vascular drugs include inhalation NO, and venous drops based on three drugs such as frontol and adenosine. It is confirmed that the study of adnotence can be replaced by adenosine. With more than ten years of clinical practice, many international medical centers are using the method of inhaling Ieloqian. Promoting, the new guide deleted adenosine as a candidate for acute drug test, and only retains three types: nitric oxide and anteronic inhalation of Ello, and intravenous pins. In fact, more and more centers, including Europe and the United States, have abandoned intravenous betae alcohol. At present, the two patterns of inhalation NO and inhaling Ielo are internationally formed internationally. 03 Early screening of lung hypertension Early diagnosis is the key to improving the treatment effect of patients with lung hypertension and long -term prognosis. It is also a clinical difficulty. The 2022ESC/ERS guide further emphasized the importance of early screening and evaluation of some specific dangerous people. Early screening specifically includes three people: 1) Non -asymptural high -risk pulmonary hypertension people, including patients with systemic sclerosis, BMPR2 mutant carriers, first -level relatives of patients with hereditary pulmonary hypertension, and patients who intend to do liver transplantation; 2) Early symptomatic patients with the risk of lung hypertension, including patients with pipeline hypertension, HIV infection patients, and non -system sclerosis connective tissue patients; 3) In order to strengthen communities and outpatient clinics with a specific population with risks of lung hypertension, including patients with a history of previous pulmonary embolism, patients with unknown reasons, etc. For patients with heart failure, whether ultrasonic heartbeat diagrams doubt whether the patient has a lung hypertension, it is important to complete the liquid or exercise load, including the cardiac catheter examination and evaluation of blood dynamics. Essence 04 Detection of right cardiac duct detection indicators of patients with lung hypertension Give specific recommendations The right cardiac duct is a key core technology for the diagnosis of lung hypertension. This version of the guideline is recommended to the blood dynamics parameters that are determined in the process of right -hearted ducts in the right heart duct of patients with lung hypertension. In addition to conventional measurement calculated body circulation and pulmonary circulation pressure, resistance and blood oxygen saturation, the guide also recommends calculation of each combination (SV), each combination index (SVI), and pulmonary arteries compliance (PAC) indicators. This has guiding significance to further standardize the operation of the right cardiac duct examination operation of pulmonary hypertension. In the past, my country's heart disease and science world attached great importance to puncture and operation, ignoring the acquisition, computing and interpretation of comprehensive hemodynamics and oxygen dynamic data. This also needs to strengthen promotion and education and training. 05 Pulmonary hypertension risk layered strategy further optimization Dangerous layers are key steps for patients with patients with pulmonary hypertension, because the current clinical treatment strategy is mainly based on different dangerous layers to make decisions. The 2015 ESC/ERS Guide proposed that the 3 classification risk layering method (low risk, medium risk, and high risk, which refers to the risk of patients' death in one year <5%, 5%~ 10%, and & 10%), including clinical symptoms, including clinical symptoms, Motor function, right -hearted functional image indicators, biomarkers and right -heart catheter indicators and other parameters, in 2018, 6th WSPH discussed at the meeting and proposed a total of 6 parameter indicators to simplify the dangerous layering method. The 2022 ESC/ERS Guide is still recommended to use the danger of the first diagnosis patients in the preliminary diagnosis patients to better associate with the severity of the disease. The main update point is to adjust the risk of death in high -risk patients from the past & 10%to & 20%, and the risk of mid -dangerous death is adjusted accordingly to 5%to 20%; other update points include: (1) Relieve the high-risk boundary value of the BNP from the past & 300 ng/L to the & 800 ng/L, while the high-risk boundary value of the NT-ProBNP is adjusted from the past & 1400 ng/L to the & 1100 ng/L; (2) Continue the ultrasonic heart dynamic diagram as an important parameter of the danger layer, increase the new variable TAPSE/Spap, & 0.32 mm/mmHg is a low -risk, <0.19 mm/mmHg is a high risk; (3) Cardiac MR increases the new variable SVI (each combination index), & 40 ml/m2 is a low -risk, <26 ml/m2 is a high risk; (4) Hematology also increases SVI (each combination index), & 38 ml/m2 is a low -risk, and <31 ML/M2 is a high risk. For the follow-up patients, it is recommended to use a quarter-class dangerous layering method, which is only included in three and the most long-term prognostic non-invasive indicators: WHO functional classification, 6-minute walking distance and BNP/NT-PROBNP. , Low and medium-risk, medium and high risks, and high risks, avoiding 60-70%of patients in the third classification method are attributed to the mid-danger, which can better reflect the relationship between danger and prognosis. 06 Patient hypertension patient treatment strategy update 1. The ESC/EESC/ERS guide in 2022 combined with new treatment strategies and evidence in recent years, it described and updated clinical treatment. In terms of overall management strategies, the guidelines are from patient's physical activity and rehabilitation exercise, anticoagulant therapy, diuretic therapy, oxygen therapy, disable left heart failure therapy drugs, anemia and iron deficiency status treatment, vaccination, psychological support and treatment compliance, etc. Multiple questions explain. Among them, the guide clearly recommends that patients with pulmonary hypertension can vaccinate the new coronal virus vaccine. Dr. Li Jingyi and Dr. Wu Xiaohan of Beijing Union Hospital are also tracking the safety of vaccination vaccine in patients with pulmonary hypertension. As a result, this recommendation plan is also supported. 2. For patients with anemia with severe iron deficiency, the guide is also recommended for iron supplementation, but the difference in the efficacy and tolerance of specific venous iron supplementation or oral iron supplementation is not clear. 3. Patients with pulmonary hypertension may face some special circumstances, such as pregnancy and contraception, surgical surgery, travel, and going to high altitude areas. Among them, for female pulmonary hypertension patients, although a small sample study reminds the prognosis of pregnancy and production of patients with pulmonary hypertension, because such patients are facing many uncertain circumstances and the production process of pregnancy will often increase the progress of pulmonary hypertension. Therefore It is still clear that doctors should fully inform female patients' pregnancy and potential risks facing. For newly found patients with pulmonary hypertension during pregnancy, if you plan to continue your pregnancy, you should avoid using endothelin receptor antagonists, Lionci and Slai Pagge with potential terators or targeted drugs with unknown toxicology. Considering the treatment of type 5 phosphate inhibitors, non -oral anterior cordin drugs or calcium channel blockers. 4. In terms of targeted therapy strategies, the new version guide has some adjustments compared with the 2015 guide. The core content includes: 1) For patients with acute pulmonary vascular dilatation tests, it is necessary to evaluate whether there are other cardiopulmonary combined diseases. For patients with non -cardiopulmonary merging diseases, initial joint treatment can be actively adopted; for patients with cardiopulmonary merging diseases, in order to avoid drug superimposed side effects, it is recommended to use single -drug oral treatment. 2) Different dangerous layered strategies for initial assessment patients and follow -up patients to guide treatment. For initial evaluation patients with comprehensive recommendation parameters, for low -risk or medium -danger patients, initial ERA+PDE5I treatment is recommended; for high -risk patients, initial ERA+PDE5I+intravenous or subcutaneous injection of front cycloid drugs; 3) During the follow -up, the 4 category recommended by the new version of the guideline simplifies the risk layered strategy. For patients with evaluation as low -risk patients to continue to maintain the original treatment; for the evaluation as a low -risk patient, you can use the prefixin receptor agonist (Silai Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pache (Silang Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa Pa's Puppet Gwang) may switch PDE5I to birdyamotenase excitement (Lisi); for patients with evaluation as high -risk or high -risk patients, add vein or subcutaneous injection of prefixin drugs or are recommended in areas with mature lung transplantation. Lung Transplantation Evaluation. 5. In terms of intervention and lung transplantation: Due to the complexity of the intervals and POTTS diversion operations, the risk of perioperative complications is high, it is recommended to be carried out in experienced central individualization; (PADN), the new version of the guidelines mentioned that the technology can improve the patient's acute and chronic hemodynamic indicators, but there is still a lack of large -scale random control research to further confirm that it needs to be further studied for the effect of receiving targeted drug treatment patients; further research; Regarding lung transplantation, if patients with pulmonary hypertension have been fully optimized, targeted therapy is still in a medium and high -risk state, lung transplantation assessment should be performed as soon as possible. The new version of the pulmonary hypertension guide has attracted widespread attention as the guidelines of other diseases, but we believe that all the authors of the European guide come from Europe, which is suitable for the reference of European clinical practice. For the actual situation in my country, we must use the actual situation of our country to flexibly use the actual situation of our country flexibly. Essence Some scholars think that we want to copy the European and American guidelines, which is undoubtedly a wrong concept. Regardless of the difference in medical insurance payment, including drugs, the differences between the people's ethnicity, the differences in the hierarchical medical system, the regional differences distributed by the high -level pulmonary vascular disease diagnosis and treatment center, the number and level of specialists will affect the clinical practice differences in China and Europe. Essence What we need to do is to criticize the absorption of the European guide, study carefully, combine our own clinical practice, update the clinical diagnosis and treatment guide of our country as soon as possible, and guide the majority of grassroots doctors to take care of patients across the country. Translate Western guidelines into Chinese, and in the era of deeds, it is gone. - END -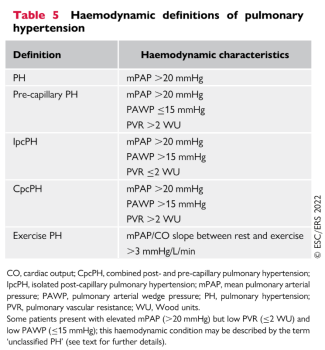

Yangjiang Municipal Committee of the CPPCC went to Dongguan Binhai Bay to investigate and exchange good strategies for development and exchange

Text/Yangcheng Evening News all -media reporter Wang MoFigure/Binhai Bay New Area ...
Fujian Zi'an: Actively respond to the demands of the masses, and comprehensively solve the "urgency and sorrow" of the masses

In recent years, Shenqiao Town has taken the demands of the masses as an important...