Breast cancer cells are "chaotic", how to choose in installments and treatment?
Author:Cancer Channel of the Medical Time:2022.09.24
*For medical professionals for reading reference

Where is it? Unclear lymph nodes? How to deal with this rare breast cancer?
Breast cancer is the most common malignant tumor among women. But the metastasis of the opposite neck is very rare to metastasize breast cancer, but there are many controversy: the exact drainage pathway? How to diagnose the staging? Should we clean the neck lymph nodes while the breast root treatment?
Recently, a case published in the BMC sub -magazine reported in detail a clinical, form, pathology, and immunohistochemical characteristics of breast cancer with the metastasis of the mammary cervical lymph node metastasis. Everyone brings inspiration ~

Study homepage screenshot
Basic cases
Patient, female, 30 years old
Prosecutor: 5 months of right breast mass, and the left neck lymphadenopathy is 5 days.
Specialty examination: There is no swelling of the thyroid gland. The left neck can be pillar and 2 swollen lymph nodes, hard, about 1.5 cm × 1.0 cm in size, and poor activity. The appearance of the bilateral breasts is normal, and the skin is not seen in the skin or dimple. The right breast can be 3 and one 3.0 cm × 2.5 cm lump. The shape is irregular, the boundary is unclear, the activity is not good, and there is no tenderness. There is no obvious mass of the left milk. Bilateral armpit lymph nodes have not seen swelling.
Imaging examination: Breast ultrasound shows a low-echoed nodule with a low breast, about 29mm × 20mm × 29mm (BR-4A). There are no obvious abnormalities in the neck ultrasound showing the thyroid gland; several low echo nodules can be seen on the left neck. Among them, there are 2 lymph -free doors in the neck III area, with 20 mm × 6 mm and 17 mm × 9 mm. Essence The ultrasonic examination of the lymph nodes on the collarbone is not obviously swollen.
Breast X-ray shows the internal quadrant of the right milk. It can be seen 33mm × 14.3 mm slightly dense lumps, accompanied by fine-like calcification (BR-4C).
MRI shows that the upper quadrant of the right breast is a swollen block, with a size of 28.8 mm × 23.5 mm × 28.9 mm, and the right axillary lymph nodes (BR-5).
PET-CT shows the increase of 2 sugar metabolites on the left chest wall on the left side of the chest and bone handle. Considering the transfer; multiple small lymph nodes in the left neck (IV area) are abnormally increased with sugar metabolism, considering multiple lymph node metastasis. (figure 1)

The whole body PET-CT: The left neck has a high-generation metabolic lymph nodes, and the left sternous handle has high metabolic nodules
diagnostic result:
1. Right breast cancer;
2. Solit -necked lymph node metastasis.
After admission, the pre -surgery was completed, and the removed right milk mass and the left neck lymph nodes were completed. During the operation, the fast pathological examination diagnosed the right breast malignant tumor and the left cervical lymph nodes low. Subsequently, the right breast removal and right axillary outpost lymph nodes were immediately performed. The fast pathological examination during the operation confirmed that the right outpost lymph node had no tumor metastasis, so the right -right armpit lymph node scanning was not performed.
Postoperative pathology: Right milk infiltration duct cancer, III grade, found an isolated tumor cell in the lymphocytes of the lymphocapoon in the first group of lymph nodes (the number of tumor cells is less than 200). There are no cancer metastasis in the two, 3, and 4 groups of outposting lymph nodes (0/3). The left neck lymph nodes have metastatic cancer (2/2). No internal cancer thromels were found. (figure 2)
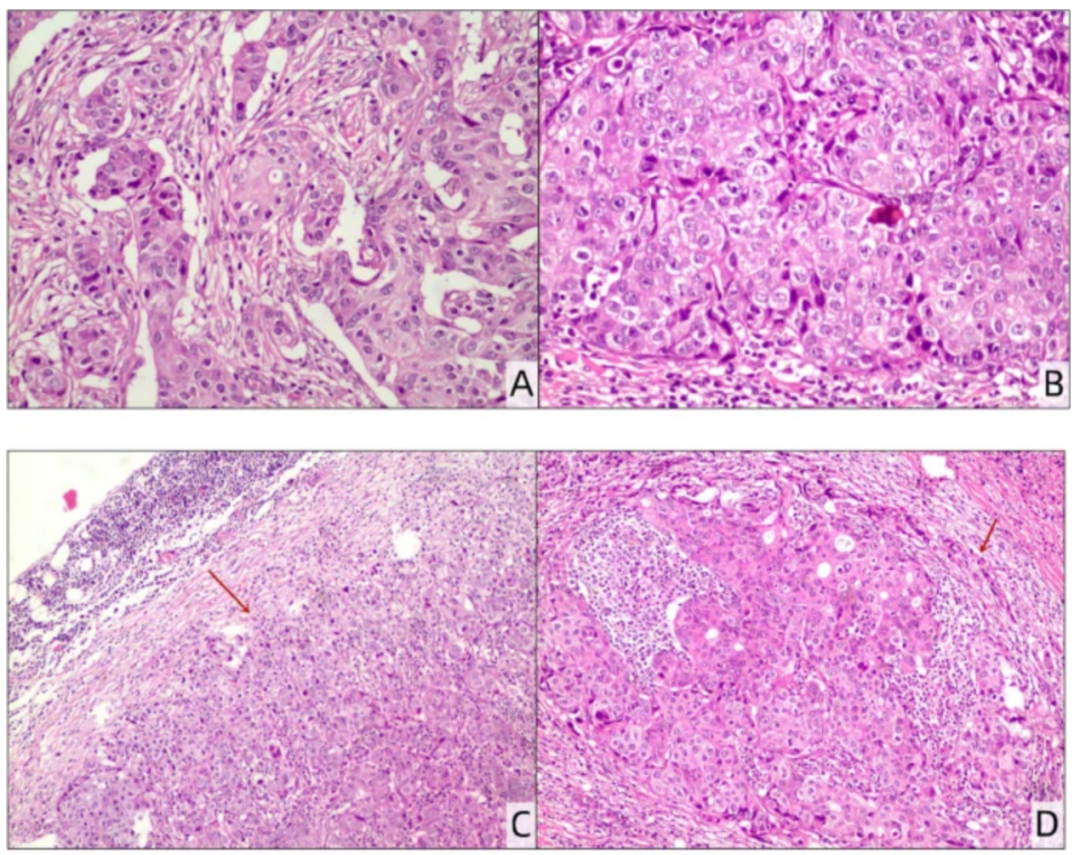
Pathological slices (A, B: HE staining, 200 ×): invasive duct cancer, level III.
Pathological slices of left -necked lymph nodes (C: HE staining, 40 ×; d: HE dye, 100 ×): Depending on cancer metastasis.
Immunization: Breast tumor cell ER (40%+), PR (5%+), HER-2 (3+), Ki67 (40%), AR (70%+), CK5/6 (−), CK7, CK7 (++), E-Cadherin (++), P63 (−), SOX-10 (−), GATA-3 (+), Mammaglobin (+), Napsin A (−), the left neck lymph node cancer cells ER (70%+), PR (20%+), HER-2 (3+), Ki67 (40%), GATA-3 (+), CK7 (++).
After surgery, chemotherapy, molecular targeted therapy, radiotherapy and endocrine therapy.
Where is the controversy: starting from the anatomy and installment
Breast cancer is very rare to metastasis on the side of the neck of the side of the neck, and the exact drainage pathway is currently controversial. The possible ways to report on literature include:
1. Digodify through the intercostal vascular skin branch to the intercostal rear lymph nodes near the rib head, and then drain to the thoracic catheter;
2. Slocked lymphatic vessels, deep lymphatic vessels under the thoracic fascia, or sternum lymphatic vessel jump to the opposite armpit lymph nodes.
To diagnose the metastasis of the lymph nodes on the side neck of breast cancer, we must also pay attention to exclude the possibility of hidden breast cancer (OBC), while considering the jump and metastasis of breast cancer. OBC should screen through ultrasound, breast X-ray photography, MRI and even PET-CT. The final diagnosis still depends on the pathology and immunohistochemistry diagnosis of metastlasia. Although the incidence of mammary cancer is relatively low in the metastasis of the lateral neck lymph nodes, breast cancer is still considered to be one of the most common metastasis to the primary malignant tumor that metastasis to the neck lymph nodes.
According to the United States Cancer Association (AJCC) (eighth edition) and breast cancer "Guidelines for the Clinical Practice of NCCN Tumor" (2020), regional lymph nodes refer to the affected axillary, up/collarbone and internal milk lymph nodes. The opposite neck lymph nodes significantly exceed the category of regional lymph nodes, and the metastasis of the opposite lymph nodes can be regarded as a distant metastasis and belongs to the IV stage. How should this rare case be treated?
Breast cancer combined with side neck lymph node metastasis belongs to the late clinical period and was once considered to be surgical taboos. The incidence of blood to the distant organs was the main cause of death after surgery. However, HONG PAN et al. Pointed out that the mammary cancer specific survival period (BCSS) and overall survival (OS) of patients with dlnm metastasis (DLNM) were similar to those of patients with lymph node metastasis (ISLM) on the same side, and local therapy and DLNM were Patient's OS improvement is significantly related. At present, domestic scholars have not yet formed consensus whether such patients should perform neck lymph nodes at the same time as breast root treatment.
BISASE B and others believe that the indicator of the cervical lymph node cleaning of breast cancer includes viable local surgical treatment of breast cancer; no remote organ metastases; armpit lymph nodes metastasis during surgery, but not affected the armpit veins; Okay, no fixed fusion.
Teshome M believes that the existence of the primary stove is undoubtedly the root cause of the distant transfer and increase the possibility of further transfer. Therefore, a certain range of surgical treatment should be performed as soon as possible, which can reduce the load of tumor and promote the treatment of chemotherapy. NCCN guidelines pointed out that patients with phase IV breast cancer should be properly treated according to the molecular type. The curative effect and opportunity of surgical resection of the primary tumor are still studying, and it is necessary to formulate an individualized solution. For some patients who have good response to initial treatment, local treatment can be considered, such as breast surgery and/or radiotherapy.
Standard electrochemical (ECT) has proven to be an effective treatment for solid tumors. A study reported that lower electric field strengths (LVHF ECT) and Palermithromy to treat recurrent breast cancer cervical lymph node metastatic patients were successful, including local control and narrowing of metastasis lymph nodes, avoiding secondary operations, and reduced reduction Standard ECT adverse reactions. Its good curative effect, safety, and tolerance make it a new treatment option for breast cancer cervical lymph nodes, especially as a secondary cervical lymph node cleansing after the root treatment of breast cancer.
references:
[1] zhong x, ding f, qian l, wu w, wen y, ding B.Breast CANCER Combined with Contractral NECK LYMPH NODE METASTASISI : 10.1186/S13000-022-01236-1.pmid: 35841040; PMCID: PMC9284882.
The first release of this article: the medical world tumor channel
Author of this article: lily
Editor in charge: Sweet
- END -
After 901 days, Xiamen International Cruise Mother Port welcomes high -end cruise ships

At 7 o'clock last night, the China Merchants Inton slowly entered from the main ch...
Clear!Perform the end of the year
On August 25, from the Shijiazhuang Social Security Center, in accordance with the relevant policies requirements of Hebei Province, Shijiazhuang City's graduates from the recruitment time from Januar...